Effectiveness of Computer Controlled Wedge Filter in Reduction of Penumbra Width in Siemens ONCOR Linear Accelerator
Ilyas N, Farrukh S, Jaffry MA
Nasir Ilyas1,4*, Salman Farrukh2 and Mishkat Ali Jaffry3
1Department of Space Science and Technology (ISST), University of Karachi, Karachi, Pakistan
2Atomic Energy Medical Centre, JPMC Karachi, Pakistan
3Department of Business Administration (IBA), University of Karachi, Karachi, Pakistan
4Department of Education and Literacy, Government of Sindh, Karachi, Pakistan
- *Corresponding Author:
- Nasir Ilyas
Atomic energy medical centre
JPMC Karachi, Pakistan
Tel: 923212026194
E-mail: Nasir.ilyaaz@gmail.com
Received Date: August 17, 2020; Accepted Date: September 02, 2020; Published Date: September 09, 2020
Citation: Ilyas N, Farrukh S, Jaffry MA (2020) Effectiveness of Computer Controlled Wedge Filter in Reduction of Penumbra Width in Siemens ONCOR Linear Accelerator. Insights Med Phys.Vol.5 No.2:8. DOI: 10.36648/2574-285X.5.2.8
Copyright: © 2020 Ilyas N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: This work discusses the variation in penumbra in presence of computer controlled wedge field as compare to open field during radiation therapy. Treatment of the target region with a remedial dose is serious for treating several cancer types; to that end, wedge filters are generally used to improve dose uniformity to the target volume. Earlier, wedges considered for this purpose were metallic/physical and were made of high-density materials such as steel or lead. Afterward, nonphysical/computer controlled wedges were introduced; these improved the dose regularity using computer systems instead of physical materials. As wedge systems develop, however, they each still have their advantages and downsides. While using metallic wedges, it is difficult to normalize the generation of secondary radiation resulting from the collision of the radiation beam with the wedge body; conversely, virtual/nonphysical wedges do not create any secondary radiation because there is no physical intervention with the radiations. On the opposite hand, virtual wedges are less suitable for treating moving tumors, like those within the lung, and physical wedges have better dose coverage to the target volume than virtual wedges.
The use of VW (Virtual wedge) is an important segment of radiotherapy the use of wedge increases the uniformity of dose in the target volume. The understanding of penumbra is essential before Treatment Planning System (TPS). Penumbra is the scattering of photon beams at the edges of collimator jaws. The aim of our study is to measure the width of penumbra width in open field (in plane direction) and in virtual wedged-field. The variation in penumbra width by introducing the PW as a function of field size, wedge angle, depth and beam energy was observed and analyzed statistically.
Materials and methods: This experiment was carried out on Siemens ONCOR impression linear accelerator (Linac). The widths of penumbra were measured by using LDA 99 detector. During our work the source to surface distance was kept 100 cm. The square field sizes on which we worked were 10 × 10 cm2, 15 × 15 cm2 and 20 × 20 cm2. Three different depth inside the water phantom Dmax (depth at which the maximum dose is obtained), 10 cm and 20 cm for the virtual wedge angles 15° and 60°, 45°, 30°. The width of penumbra are taken for both photon energies 15 MV and 6 MV, tissue equivalent water phantom IBA blue water phantom inside which all the observations were taken. The width of penumbra in virtual wedged field is subtracted from the penumbra width in open field in in-plane direction. The variation in penumbra width as a function of beam energy, field size, depth and wedge angle were analyzed statistically by using statistical package for social sciences (SPSS).
Results: Analysis of variance (ANOVA) shows that the mean variation in the penumbral width is not significant statistically with the change in depth and beam energy, statistically significant with the change in field size and highly significant with the change in wedge angle.
Conclusion: Our study gives the statistical significance of wedge angle, field size, depth and beam energy on penumbra reduction in presence of virtual wedges. This study is useful in treatment planning in different virtual wedge angles, depth, field size and beam energy. This also describes why VW is better to use in reduction of penumbra width.
Keywords
Variations; Penumbral width; Virtual wedge
Background
In ocular therapy, wedges are used in order to auxiliary a critical tissue, e.g. macula or optic disc, or more usually, to lessen the high dose volume. Approximately half of practicing ocular proton therapy centre employ wedges [1]. During recent radiotherapy the heart toxicity and breast cancers are becoming major issues [2]. Radiotherapy of breast has always been challenging in terms of the range of sizes and shapes of breast volumes as well as the vicinity of the whole-breast volume to the surrounding critical organs. One of the intrinsic challenge when planning whole-breast radiation therapy is the reality that treatment is somewhat limited to what is really a different technique in order to avoid these surrounding critical organs [3].
In most of patient radiations associated cardiac diseases have been commonly found which were treated for lymphoma, breast cancers, seminoma, peptic ulcer diseases and lung cancer and also in the persons who survived in atomic bomb explosion [4]. The risk of cardiac diseases may be related to both radiation and irradiated volume [5]. Quality of a radiation beam is most usually expressed in terms of its penetrating power, which is mainly a function of the mean photon energy and it may be fully defined by its depth dose characteristics in water but an rise in the surface dose with the field size is also eminent due to the electron scattering from intervening materials [6]. It is necessary to have the knowledge and understanding of use of wedge filter during Treatment planning system (TPS) because it becomes more necessary to weaken radiation toxicity. While treating thoracic, breast and pelvic tumors the insertion of wedge filter is common and the steep dose slope may produce hot spots in hearts, lungs, and rectum in these cases [7-9].
Penumbra is important beam characteristics parameters which are defined as the distance between 80% and 20% points of dose on a transverse beam profile. In common the term penumbra means the region at the edge of a radiation beam, over which the rate of dose changes quickly as a function of distance from the central axis. The physical penumbra is the sum of individual geometric penumbra and transmission penumbra and it is mostly due to the scatter in medium [10]. Variation in the dose at the edges of the beam caused by collimator is called transmission penumbra. The factor produces transmission penumbra is the different thickness of collimator blocking the beam and its occurrence is due to the beam energy from the edges or the blocks. On the other hand, the geometric penumbra is width of the penumbra at any depth due to geometry of setup. Geometric penumbra occurs due to the size of source, large sources have large geometric penumbra. Scatter penumbra is produced under collimator jaws into the region of penumbral tail; there is a little bit of dose produced by the jaws of collimator [10]. The physical penumbra is affected by the beam energy, finite source size, source to surface distance (SSD), source to collimator distance (SCD) and depth in the water phantom [4]. Penumbra creates higher doses than normal at the edges of tissues which are not unwanted. For a steep dose gradient between the irradiated volumes and healthy tissues, the penumbral width should be as small as possible. In order to reduce penumbral width the diameter of source should be minimum. The diameter of source should be 2-3 mm for recent linear accelerators. Penumbra can be reduced by increasing the source to collimator distance (SCD) and by using secondary blocks placed near to the patients for shaping the field [11]. Penumbra can be compact by strengthening the clearance between irradiation head to surface/skin in order to using wedge filters. It indicates that penumbra also depends upon the direction of collimator edges. The leaves of collimator always are directed towards the source and autonomous position of leaf, this property is named as focusing. Focusing can be obtained by the movement of leaves in circular path or by the rotations of the edges of leaf [12]. For this reason MLCs (Multileaf collimators) curved edges are utilized in modern LINACS. But in case of curved leaves penumbra is not completely independent of leaf position [13]. As far as the clinical advantages or disadvantage is concern the penumbral region needs requires attention during treatment planning. Penumbra of the beam is not considered when delineating the PTV Planning Target Volume (PTV), clinical target volume (CTV) and gross tumor volume (GTV), however when selecting the beam sizes, the width of the penumbra has got to be taken under consideration (Figure 1). Here we are able to conclude, penumbra plays an immense role in dose delivery accuracy for radiation. For treatment planning, penumbra width and force field off set strongly effect target dose conformity and organ at risk sparing [14].

Figure 1: Shows the ICRU 50 measurements volume [15].
Intrafractional organ motion (tumor motion) is a noticeable problem in radiotherapy [16]. Tumor movement can be produced by the skeletal muscular, respiratory, cardiac, and gastrointestinal systems. Respiratory motion in particular affects all tumor sites in the thorax and abdomen; the disease of most significant in this case is lung cancer. Respiratory motion is just one potential source of error in radiotherapy [17]. Intrafractional organ motion may result in two sorts of effect” which results in the under/over dose to the irradiated tumor one of the major cause of dose blurring is the wedge angle variation from actual one. Second is called the “interplay effect,” which is only an obstacle in the case of vibrant delivery of intensity-modulated radiation therapy or dynamic treatments with computer controlled wedges. This influence is the result of interaction between the moving tumor and the motion of the radiation beam as defined by the computer control wedges and can result in dose variation [18,19].
The variation within the penumbra needs to implement during TPS especially it creates problem in delivering small off-center segments.
Tissues closer to the edges of field have greatest dose uncertainties and correct measurement is required of the spatial dose variation with the limitation of computer controlled algorithm. Mega volt photon beams produce a high increase in dose in a few mm of tissues and organs [20]. For intensity modulation radiation therapy (IMRT) which delivered through MLCs, beamlet dose intensities can be changed by stirring the MLC leaves with in the irradiated field; therefore, accurately modelling penumbra and transmission for the MLC leaves is very important [21]. In this work the comparison of penumbral dose for open field and virtual wedge filter is carried out. The key purpose of this study is to look at the behaviour of penumbra of open filed and virtual wedge fields at various wedge angles, depth, and energy and field size.
Materials and Methods
All the measurements were taken on Siemen’s ONCOR Linac having 82 Leaves MLC as X-collimator. In the commissioning of TPS, the beam data for wedge field needs to be more precise because minor instability can cause greater impact in clinical setting due to dose gradient profile. Because of different techniques use to generate wedged dose distribution and their positions with respect to the target of Linac, the virtual wedge (PW) are expected to have some different dosimetric characteristics [22].
The virtual wedge is a software/hardware system that allows delivery, during radiation therapy treatment, of a wedge shaped dose distribution without the use of a physical wedge. It produces a dose distribution without the use of physical wedge by varying beam intensity while moving a collimator jaw at constant speed across the treatment field. Virtual wedge is also called dynamic wedge in different vender of Linac. The virtual wedge could be of any range (i.e. 10° to 60°) and possible for in and out direction. The basic dosimetric principles of the Siemens virtual wedge are presented by Santvoort et al. in 1998 [23]. In early years, digital LINAC has made it possible to create wedged dose distributions through collimator motion which was totally controlled by computer algorithm. The report of first implementation of dynamic wedge (DW) by Leavitt et al in 1990 [24], Recently, Siemens has introduced a VW that creates dose distribution similar as created by wedge through the motion of one of the collimator jaws across the field during irradiation. For a certain VW field, the speed of the jaw motion is constant but the dose rate changes. VW was designed to produce dosimetric properties same as of physical wedges (PWs) [25].
Virtual wedge treatments begins with an initial gap jaw configuration to optimize dose distribution to the ‘toe’ edge of the field .Because of dynamic jaws over travel limitations ,the programming of certain fields may results in a large initial gap. An initial gap greater than 1.5 cm may result in an open field effect at the “toe” edge of the field. This system will automatically move the dynamic jaw to its starting point, leaving a gap between the jaws referred to as the initial gap [26]. A wedge profile is obtained by controlling the movement of one of the secondary jaws as well as varying the dose rate at the time of irradiation [27]. The dose rate is varied according to the following equations [28].
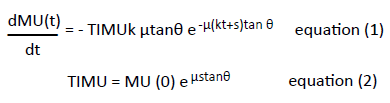
Where
MU(0)=Monitor unit set on the central axis
S=Distance of stationary jaws from central axis
μ=Water’s linear attenuation coefficient at beam energy
K=Speed of moving jaw
θ=chosen wedge angle
When treatment has been entered and accepted on a LINAC console, the monitor displays a curve which specifies the final positions of moving and stationary jaws as well as the dose to be delivered at each point across the field with respect to prescribed MUs on central axis. TIMU is the position of jaw at rest. The highest monitor unit shown on this curve is at the position of stationary jaws.
As treatment set-up parameters accepted, the dynamic jaw moves to its initial position close to the opposite stationary jaw without touching it. During treatment, the dynamic jaw moves at a constant speed to its final position but the dose rate varies. This produces the required wedge profile by delivering higher dose at the “toe” of the wedge field as compare to the “heel” during the dynamic phase of treatment .It is clear from equation (1) and (2) that an random wedge angle can be obtained.
The collimator system on the Siemens ONCOR is equipped with a multi leaves collimator (MLC) as X-jaws, so the VW is only implemented in the direction of Y-Jaws (upper jaws) which is non MLC direction. The bottom of the Y jaws is at 30.1 cm below the target. For each Y jaws, the highest open position of the jaw is 20 cm, and the maximum over travel, travel past the central axis is 10 cm.The range of speed of Y jaws raging from (0.2-15) mm/sec [26].
Atomic energy medical center (AEMC), Karachi where Linac installed for both 15 MV and 6 MV X-ray beams using 3D water phantom (Blue phantom, IBA Germany). The dimension of water tank is 480 mm × 480 mm × 400 mm and walls are made of acrylic. Water phantom has point accuracy about 0.1 mm with 500 mm/s scanning speed. We align the water phantom with the laser such that the vertical axis (y-axis/In-plane direction) is the in-out/gun target position. The scanning the orientation in gun target direction can compromise the TPS of wedged field, but in open field orientation does matter. For accurate scanning process, the phantom must be positioned so that it is adjusted with in-cross-plane direction. This can be carried out by aligning probe holders with the edge of fields. Standard relative dosimetry setup was arranged for measurement, using LDA-99 detectors,, portable IBA electrometer/control unit, and CU-500E and dosimetry computer having Omnipro accept software. LDA 99 was kept at beam’s central axis, with chamber center at water surface, such that the distance from source to surface (SSD) was 100 cm. Cross plane beam profiles were measured at three different depths (Dmax, 10 cm, 20 cm) for different field sizes (10 × 10 cm2, 15 × 15 cm2, 20 × 20 cm2) for open field (inplane). All the profiles then converted into tabular form using special option in the Omnipro accept software. Penumbral width for all cases (open field and virtual wedge field) was calculated by beam profiles. Penumbral width variations were obtained by subtracting the penumbral width in VW field from open field (In-Plane) direction. All the variations were finally analyzed as a function of field size, wedge angle, energy and depth by using statistical software package SPSS15. If variations are positive means penumbral width in open filed are greater than penumbral width in wedge field and negative deviations shows vice versa.
Results and Discussion
Table 1 shows the difference in penumbral width between open and virtual wedged field for all selected wedge angles, field sizes and depths.
| Energy (MV) | Depth (cm) | Field sizes (cm2) | Variations | |||
|---|---|---|---|---|---|---|
| 6 | PW 15° | PW 30° | PW 45° | PW 60° | ||
| Dmax | 10 × 10 | 0.2 | 0.5 | 0.9 | 1.4 | |
| 15 × 15 | 0.1 | 0.6 | 1.2 | 2 | ||
| 20 × 20 | 0.7 | 1.5 | 1.5 | 3.2 | ||
| 10 | 10 × 10 | 1 | 1.2 | 1.5 | 2 | |
| 15 × 15 | 1.9 | 2 | 2.1 | 1.9 | ||
| 20 × 20 | 1.9 | 2.3 | 1.1 | -4.2 | ||
| 20 | 10 × 10 | 1.6 | 1.9 | 2.2 | 2.4 | |
| 15 × 15 | 3 | 1.9 | 0.6 | -3.5 | ||
| 20 × 20 | 1.2 | -1 | -5.6 | -15.8 | ||
| 15 | Dmax | 10 × 10 | 0.4 | 0.9 | 1.6 | 2.7 |
| 15 × 15 | 1.7 | 2.3 | 2.5 | 2.2 | ||
| 20 × 20 | 2.6 | 1.9 | 1.8 | 1.8 | ||
| 10 | 10 × 10 | 0.9 | 1.1 | 1.5 | 2 | |
| 15 × 15 | 1.5 | 2.2 | 2.3 | 2.2 | ||
| 20 × 20 | 1.5 | 2 | 1.9 | 0.4 | ||
| 20 | 10 × 10 | 1.4 | 1.7 | 2.1 | 2.6 | |
| 15 × 15 | 2.2 | 2.7 | 2.3 | 1.2 | ||
| 20 × 20 | 2.6 | 1.9 | 1 | -2.7 | ||
Table 1: Deviation in the penumbral width between open and Physical wedged field.
Figures 2 and 3 shows that the penumbral deviations is positive in all cases means presence of PW decreases penumbral width especially in 60° the wedge field for larger field sizes.

Figure 2: Represents variations in penumbral width in presence of virtual wedge for 6 MV energy (a) Dmax (b) 10 cm (c) 20 cm.

Figure 3: Represents variations in penumbral width in presence of virtual wedge for 15 MV energy (a) Dmax (b) 10 cm (c) 20 cm.
As far as energy of x-rays beam concerned the mean variation negative in 6 MV x-rays energy whereas positive in 15 MV energy, it shows that in the presence of low energy VW has greater penumbra than open field and in high energy vice versa. Radiation therapy not only destroys or slows the expansion of cancer cells, it can even affect neighbouring healthy cells (Table 2). Damage to healthy tissues can cause side effects. In external beam radiation therapy where tumor needs low energy to kill the deoxyribonucleic acid (DNA), we must ensure the secondary radiations produced by the movement of collimator jaws. The beam hardening effect produces the higher penumbra width in presence of VW in low energy treatment. In high energy treatment penumbra or scattering from the jaw of collimator reduces. High-energy radiation damages inherent material of cells and thus disruptive their ability to divide and proliferate further [29]. As P value is greater than 0.05 which shows that statistically not significant but medically it can be significant in low energy interference. The beam energy has been already reported to affect the penumbra to the external beam photon radiotherapy [30]. Most of lung cancer patients who undergo radiation therapy are treated with higher-energy photons such as 10 MV or higher to obtain a deeper penetration and well dose uniformity. Lung cancer leftovers the leading cause of cancer death in United States, and existence for locally advanced non-small cell lung cancer (NSCLC) remains limited at around 30% at 5-years [31]. However, lower energy such as 6 MV photon beams should be preferred over higher energies photons because of the significant loss of lateral dose equilibrium for high-energy beams in the low density medium [32].
| Factors | Categories | N | Mean Variation | Standard Deviation | F-Value | P-Value |
|---|---|---|---|---|---|---|
| Energy | 6 MV | 36 | -0.139 | 4.2076 | 1.908 | 0.172NS |
| 15 MV | 36 | 0.958 | 2.2376 | |||
| Depth | Dmax | 24 | 0.954 | 1.285 | 0.537 | 0.587NS |
| 10 cm | 24 | 0.333 | 4.2807 | |||
| 20 cm | 24 | -0.058 | 3.8707 | |||
| Field Size | 10 × 10 cm2 | 24 | 1.342 | 0.5492 | 3.04 | 0.05 * |
| 15 × 15 cm2 | 24 | 0.796 | 2.8832 | |||
| 20 × 20 cm2 | 24 | -0.908 | 4.9003 | |||
| Wedge angle | 15° | 18 | -2.611 | 5.5162 | 8.349 | 0.000* |
| 30° | 18 | 1.467 | 0.8303 | |||
| 45° | 18 | 1.533 | 0.8758 | |||
| 60° | 18 | 1.25 | 1.7939 |
Table 2: Factors affecting penumbral deviations statistically.
In case of water Phantom depth the mean variation in dmax is higher and positive and at 10 cm depth it is also positive but lesser than dmax. If we go further deep i.e. 20 cm deviation becomes negative it shows in 20 cm VW has higher penumbra width. The width of penumbra increases in virtual wedge fields [9], depth losses the energy of photon so scattering increases in deep cancer sites such as prostate, lung and esophagus, we must make sure the radiation toxicity before TPS. This effect is not statistically significant.
As far as the size of field is concerned, the penumbra variations are greater and positive in 10 × 10 cm2 , it means that penumbra width in open field is greater than VW field in this field size. the variation is also positive in 20 × 20 cm2 field size but lesser than lower field size. The variations in penumbra becomes negative in 20 × 20 cm2 field sizes i.e. penumbra width increases in presence of VW in deep sites. Peripheral doses outside the geometric projection of VW treatment field is increases as compare to open field [21]. This effect is statistically significant, we must consider the outside peripheral doses before treating large size tumors.
Penumbra increases with depth and remain negative i.e. width of penumbra reduces as we introduce PW. It shows that in depth the scattering of photon beam reduces which reduce the penumbra depth in presence of metallic wedges this factor increases the deviation in penumbra. This effect is statistically significant as p value is 0.05 .The reduction of penumbra width has been notice previously [30]. In treating deep cancer sites such as prostate, lung and esophagus, we must make sure the radiation toxicity before treatment planning system.
In case of wedge angle the variation is negative in 15° VW. In other considered angles the variation is positive it means penumbra width decreases in the presence of VW. In case of small angle such as 15° wedge the variations are negative due to the photons scattering from the moving jaw. In case of large angle wedges the scattering decreases which reduce the penumbral width in virtual wedges so all deviations are positive as wedge angle increases penumbra width decreases this is an importing factor to know before treatment planning system or in steep cancer treatment. The effect of small-angle proton scatter from the edge (toe) of a wedge partially placed has been noted earlier [33]. Statistically this is highly significant and in most clinical site is has ample importance such as 3D intensity modulation radiation therapy [34-36].
Conclusion
Penumbra width produces higher doses than normal at the edges of tissues which are adverse. The penumbral width should be as small as possible between the target volume and healthy tissues for a steep dose gradient. As far as the clinical importance or disadvantage is concerned, the penumbral region requires defined attention during treatment planning. When describing the planning target volume (PTV), clinical target volume (CTV) and gross tumor volume (GTV), Penumbra of the beam is not considered, however when selecting the beam sizes, the size of the penumbra has to be taken into account. The CTV is significant because this volume must be effectively treated to make cure. The variation in the penumbra has to be executed during TPS especially it produces problem in delivering small off-center segments. This study is very supportive to know the penumbral dose variation of open field, physical wedge field and hence its application in accurate commissioning and clinical use.
It is a well-known fact that due to improved use of advance radiotherapy techniques like intensity modulation radiation therapy (IMRT), Volumetric modulated arc therapy (VMAT), Stereotactic radiation therapy (SRT) etc., and where the specialists are debating that hard wedges in radiotherapy should be withdrawn. There are most of less developing countries in world like Pakistan are still lots of radiotherapy centers having lack of resources, and they are using hard wedges and EDW/Virtual wedges so it is important to check periodical wedge profile reproducibility. The model and understanding of this study will also be valuable in case of IMRT delivery where the leakage penumbra effect of MLCs should be taken into account for accurate dose calculation. Our study gives describe in which conditions undesirable penumbra width increases and how to manage it. In most of the cases penumbra width in VW decreases and best to use in most clinical site depends upon its availability.
References
- Baker C, Kacperek A (2016) The influence of physical wedges on penumbra and in-field dose uniformity in ocular proton beams. Phys Medica 32: 1-6.
- Darby SC, Ewertz M, McGale P, Bennet AM, Blom-Goldman U, et al. (2013) Risk of ischemic heart disease in women after radiotherapy for breast cancer. New Engl J Medicne 368: 987-998.
- Small K, Kelly C, Beldham-Collins R, Gebski V (2013) Whole breast and excision cavity radiotherapy plan comparison: Conformal radiotherapy with sequential boost versus intensity-modulated radiation therapy with a simultaneously integrated boost. J Med Radiat Sci 60: 16-24.
- Wolfgang S, Thomas B, Grosu AL (2006) New Technologies in Radiation Oncology.
- Gagliardi G, Constine LS, Moiseenko V, Correa C, Pierce LJ, et al. (2010) Thorax: Heart radiation dose-volume effects in the hear. Int J Radiation Oncology Biol Phys 76: 77-85.
- Kastrati L, Nafezi G, Shehi G (2016) The penumbra of irradiations in linear accelerators, its use in radiotherapy of cancer diseases, negative effects and the possibilities of reducing them. RAD Conference Proceedings 1: 111-113.
- Bhatnagar AK, Brandner E, Sonnik D, Wu A, Kalnicki S, et al. (2006) Intensity modulated radiation therapy (IMRT) reduces the dose to the contralateral breast when compared to conventional tangential fields for primary breast irradiation. Breast Cancer Res Treat 96: 41-46.
- Ling T, Slater J, Nookala P, Mifflin R, Grove R, et al. (2016) Analysis of intensity-modulated radiation therapy (IMRT), proton and 3D conformal radiotherapy (3D-CRT) for reducing perioperative cardiopulmonary complications in esophageal cancer patients. Cancers 6: 2356- 2368.
- Farrukh S, Ilyas N, Naveed M, Haseeb A, Bilal M, et al. (2017) Penumbral dose characteristics of physical and virtual wedge profiles. Int J Med Phys Clin Eng Rad Oncol 6: 216-224.
- Pdgorsak EB. Radiation oncology physics: A hand book for teachers and students (International Atomic Energy Agency, Vienn, 2005).
- Khan FM. Lippincott Williams & Wilkins (2003) 3rd edn. Physics of radiation theraphy.
- Pastyr O, Echner G, Hartmann GH, Richter J (2011) Dynamic edge focussing: a new MLC-design to deliver IMRT with a double focussing high precision multi-leaf collimator. J Radiother Med Oncol 61: 624-643.
- Butson MJ, Yu PKN, Cheung T (2003) Rounded end multi-leaf penumbral measurements with radiochromic film. 48: 247-252.
- ZhouD, Zhang H, Ye P (2015) Rounded leaf end effect of multileaf collimator on penumbra width and radiation field offset: an analytical and numerical study. Radiol Oncol 3: 299-306.
- Landberg J, Chavaudra T, Dobbs J, Hanks J, Johansson G, et al. (1993) Reports of the international commission on radiation units and measurements. J Int Comm 26: 1-2.
- Akasaka H, Mukumoto N, Nakayama M, Wang T, Yada R, et al. (2017) A comparison of physical vs. nonphysical wedge modalities in radiotherapy. Radiother 1: 8-10.
- Keall PJ, Mageras GS, Mageras JM, Mageras RS, Mageras M, et al. (2006) The management of respiratory motion in radiation oncology report of AAPM task group 76 a). Med Phy 33: 3874-3900.
- Isa M, Iqbal K, Afzal M, Buzdar SA, Chow J (2012) Physical and dynamic wedges in radiotherapy for rectal cancer: a dosimetric comparison. Med Phys 39: 4636.
- Pemler P, BessererJ, Lombriser N (2001) Influence of respiration-induced organ motion on dose distributions in treatments using enhanced dynamic wedges. Med Phys 28: 2234-2240.
- Pam Cherry. (Wiley-Blackwell, 2009) Practical radiotherapy: physics and equipment, 2nd edn.
- Chow JC (2016) Leakage-penumbra effect in intensity modulated radiation therapy step-and shoot dose delivery. World J Radiol 8: 73-81.
- Ilyas N, Farrukh S, Iqbal J, Abdul S, Ahmad H (2016) Wedge factor dependence on computer controlled wedge system in siemens ONCOR linear accelerator. Med Phys 3: 66-72.
- Santvoort JV (1998) Dosimetric evaluation of the siemens virtual wedge dosimetric evaluation of the siemens virtual wedge. Phys Med Biol 43: 2651-2663.
- Leavitt DD, Martin M, Moeller JH (1990) Dynamic wedge field techniques through computer controlled collimator motion and dose delivery. Med Phys 1: 87-91.
- Barderoma RD, Bjärngard BE (2004) The relation between wedge factors in air and water. Med Phys 21: 1043-1047.
- Zhu XR, Gillin MT, Jursinic PA, Lopez F, Grimm DF (2000) Comparison of dosimetric characteristics of siemens virtual and physical wedges. Med Phys 27: 2267-2277.
- Saminathan S, Manickam R, Supe SS (2012) Comparison of dosimetric characteristics of physical and enhanced dynamic wedges. Reports Pract Oncol Radiother 17: 4-12.
- Attalla EM, Abo-Elenein HS, Ammar H, El-Desoky I, Ammar H (2010) Association of medical physicists of india comparison of dosimetric characteristics of siemens virtual and physical wedges for ONCOR linear accelerator. J Med Phys 35: 129-186.
- Jackson SP, Bartek J (2009) The DNA-damage response in human biology and disease. Nature 461: 1071-1078.
- Oh SA, Kang MK, Yea JW, Kim SK, Oh YK (2012) Study of the penumbra for high-energy photon beams with gafchromic TM EBT2 films. J Korean Phy Soc 60: 1973-1976.
- Zou Z, Bowen SR, Thomas HMT, Sasidharan B, Rengan R, et al. (2019) Scanning beam proton therapy versus photon IMRT for stage III lung cancer: comparison of dosimetry, toxicity and outcomes. Int J Radiat Oncol 105: 540.
- Tang SQ, Jen YM, Wu JM (2019) An empirical model for describing the small field penumbra in radiation therapy. BioMed Res Int 2019: 1-3.
- Carnicer A, Angellier G, Thariat J, Sauerwein W, Caujolle JP, et al. (2013) Hérault quantification of dose perturbations induced by external and internal accessories in ocular proton therapy and evaluation of their dosimetric impact. Med Phys 40: 1-12.
- Burnet NG (2004) Defining the tumour and target volumes for radiotherapy. Cancer Imag 4: 153-161.
- Njeh CF, Suh TS, Orton CG (2016) Radiotherapy using hard wedges is no longer appropriate and should be discontinued. Med Phys 43: 1031-1034.
- Kirkby C, Ghasroddashti E, Angers CP, Zeng G, Barnett E (2017) Comp reports and documents comp report : CPQR technical quality control guideline for medical linear accelerators and multileaf collimators. Med Phys 19: 22-28.

Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences